The clinical utility of Neuropharmagen® has been evaluated in several clinical studies that have been published in peer-reviewed journals. Our continuous efforts in precision medicine include additional clinical studies with Neuropharmagen® currently underway.
Randomized, double-blind, controlled, naturalistic, multicentric, prospective clinical trial that enrolled 316 patients with major depressive disorder
The first large randomized controlled trial (RCT) with a pharmacogenetic-based decision support tool on patients with major depressive disorder, conducted in 18 hospitals in Spain.
Designed to evaluate the efficacy of Neuropharmagen® in the choice of drug treatment, measured by the Patient Global Impression of Improvement scale (PGI-I).
Main Endpoint: The primary variable was the number of patients responding to treatment, which was defined as those who indicated that they felt “Moderately better” or “Much better” on the Patient Global Impression of Improvement scale (PGI-I). Secondary variables such as the Hamilton Depression Scale (HDRS-17) or the FIBSER (Frequency, Intensity, and Burden of Side Effects Ratings) were also analyzed to assess the tolerability of the treatment.
Results
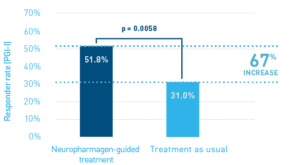
The use of Neuropharmagenzsup>® increased the response rate among patients with 1 to 3 therapeutic failures by 67%, after 12 weeks. OR: 2.39 [CI: 1.28-4.44].
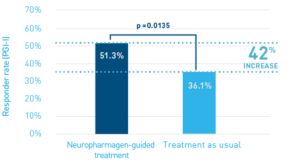
Treatment response rate was significantly increased after 12 weeks in the Neuropharmagen® -guided group, compared to patients treated as usual. OR: 1.86 [CI: 1.13-3.05].
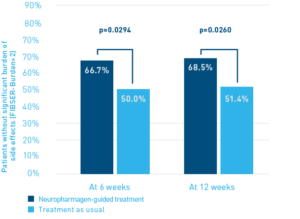
The burden of adverse effects was significantly decreased in the Neuropharmagen® -guided group, compared to patients treated as usual. Rate of patients with significant burden of adverse effects after 6 weeks and after 12 weeks. OR: 0.50 [CI: 0.27-0.94] and OR: 0.49 [CI: 0.26-0.92], respectively.
This is a reanalysis of clinical data obtained in the AB-GEN randomized clinical trial (post-hoc analysis) to evaluate the clinical utility of pharmacogenetic-guided therapy with Neuropharmagen® in specific patient subpopulations according to age, baseline severity and duration of the depressive episode.
Design: Prospective, double-blind, randomised clinical trial in patients with major depressive disorder (MDD). See AB-GEN study.
Main Endpoint: To investigate the impact of factors shown to influence antidepressant response (such as age, baseline severity and duration of the depressive episode) in the clinical utility of Neuropharmagen®. Endpoints considered were PGI-I response (score of ≤ 2), HDRS score change and HDRS response (change ≥ 50%).
Subjects: The study population was described in the main publication of the AB-GEN study results. In this reanalysis of data, the following patient subpopulations are studied: Age (< 60 years old; 60 years and older), baseline severity (baseline HDRS < 18; baseline HDRS ≥ 18; baseline HDRS ≥ 25); time from diagnosis (up to 1 year; up to 5 years; more than 5 years).
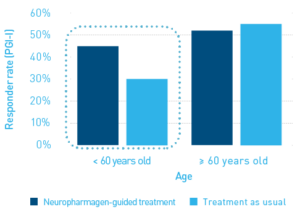
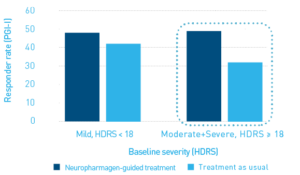
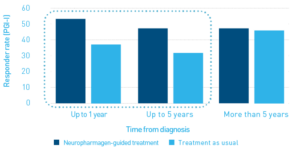
Results: PGx-guided treatment significantly improved response rates in non-aged patients compared to TAU (below 60 years old; same results were obtained with < 65 years cut-off), in subjects with moderate-to-severe depression, and in patients with diagnoses up to 1 and up to 5 years old. Subpopulations in the reanalysis were reasonably balanced regarding demographic and clinical characteristics, with an evenly distributed number of individuals between the PGx-guided and treatment-as-usual (TAU) arms.
PGI-I results according to patient age (<60 years, p=0.015; >o=60 years, p=0.813)
PGI-I results according to main severity (mild, HDRS < 18, p=0.638; moderate+severe, HDRS>o= 18, p=0.031)
PGI-I results according to time since diagnosis of MDD (under 1 year, p=0.043; under 5 years, p=0.019; over 5 years, p=0.891)
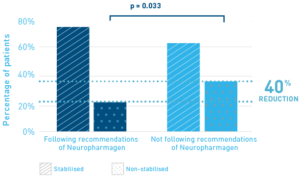
Design: Observational, naturalistic, cross-sectional, multi-centric, retrospective study. All patients had been assigned an initial medication per standard medical practice, and the Neuropharmagen® test was performed for all subjects.
Main Endpoint: To determine the association between the pharmacogenetic profile (as determined by Neuropharmagen®) and clinical evolution at 3 months, comparing subjects whose treatment was decided based on the test results and subjects whose treatment was decided regardless of the test results. Clinical evolution was measured by means of the Clinical Global Impression of Severity score (CGI-S). Stabilization was defined as CGI-S ≤3 at 3 months.
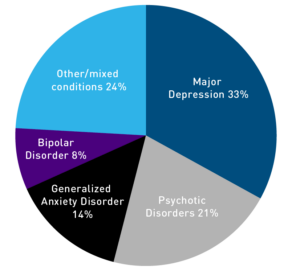
Subjects: 191 patients with affective or psychotic disorders according to DSM-IV whose previous treatment had failed, with CGI-S ≥ 3 (92% had CGI-S ≥ 4) at baseline and having detailed information about their therapeutic regime were included in the analysis (see STROBE2007-compliant subject flow below).
Results: The use of Neuropharmagen® helped reduce the percentage of non-stabilized patients by 40%, regardless of the psychiatric diagnosis.
Randomized, single-blind, controlled, multicentric, prospective clinical trial in 100 patients with major depressive disorder
The first non-industry sponsored trial of a pharmacogenetic-based decision support tool for psychiatry in a cohort of Asian descent.
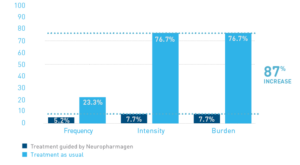
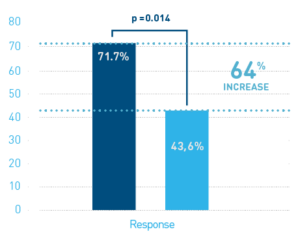
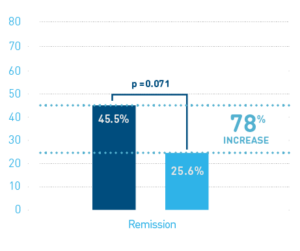
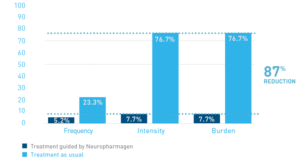
Designed to evaluate the effectiveness and tolerability of Neuropharmagen®-guided treatment in Korean patients based on Hamilton Depression Rating Scale-17 (HDRS-17) score change and Frequency, Intensity, and Burden of Side Effects Ratings (FIBSER) score change, respectively.
Response rate (%) defined according to a 50% reduction in the HDRS-17.
Remission rate (%) defined as a HDRS-17 score < 7 after 8 weeks.
Rate of Patients with significant frequency, intensity, and burden of side effects (%) after 8 weeks, defined according to the Frequency, INtensity and Burden of Side Effects Rating (FIBSER) score of > 2
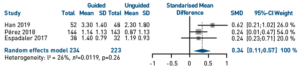
A meta-analysis of the clinical studies that had examined the effect of Neuropharmagen® on the improvement of adult patients with major depressive disorder was performed.
Design: A total of 450 eligible subjects from three clinical studies were examined. Random effects meta-analysis was conducted. Standardized mean differences (SMD), and their respective 95% confidence intervals (CIs), were calculated from clinical response data (CGI-S and HDRS-17 score change) for each individual study as well as the combination of all. Odds-ratios (ORs) were estimated from standardized differences in the continuous variables analyzed (CGI-S and HDRS-17 score change) using the logistic approximation method developed by Hasselblad and Hedges.
Results: The random effects model estimated a statistically significant effect size for the pharmacogenetic-guided prescription (d = 0.34, 95% CI = 0.11-0.56, p-value = 0.004), which corresponded to approximately a 1.8-fold increase in the odds of clinical response for pharmacogenetic-guided vs. unguided drug selection. After exclusion of patients with mild depression, the pooled estimated effect size increased to 0.42 (95% CI = 0.19-0.65, p-value = 0.004, n = 287), corresponding to an OR = 2.14 (95% CI = 1.40-3.27). These results support the clinical utility of this pharmacogenetic-based tool in the improvement of health outcomes in patients with depression, especially those with moderate-severe depression.
Fold increase in the odds of clinical response with Neuropharmagen®
Individual and pooled effect sizes for clinical response based on CGI-S score change
Prospective, observational, naturalistic study in 30 bipolar patients
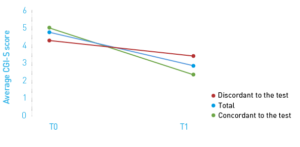
Designed to examine the role of pharmacogenetic testing in the treatment of patients suffering from bipolar disorder comparing patients that received a therapeutic change consistent with PGx-testing with patients that maintained a therapy discordant with the test results based on clinical status using CGI-S, HDRS-21 and YMRS scales and adverse events recorded with the DOTES scale.
Evolution of severity was more favorable in patients whose therapy had been changed accordingly to the test results.
A normalization in the number of adverse effects occurred in the group following the test recommendations.
Clinical Global Impression Severity-S) average scores at baseline (T0) and 3-month follow-up (t1).
Designed to evaluate the possible cost savings derived from the use of a pharmacogenetic test in bipolar patients.
The comparison of costs before and after the change of therapy according to the recommendations of Neuropharmagen® resulted in cost savings in terms of number of hospitalizations, as well as the average duration of hospitalizations.
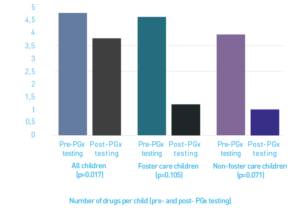
Design: Retrospective cohort study of children and adolescents with severe mental disorders who received treatment and underwent PGx testing. Proportion of patients achieving clinical improvement (CGI scale), amelioration of side effects (self-reported) and changes in the number of drugs prescribed were evaluated.
Subjects: 20 children and adolescents that underwent pharmacogenetic testing with Neuropharmagen® (10 living in residential foster care; and 10 who were not). 13 (65%) were on polypharmacy. All patients were 17 years or younger.
Results: Pharmacogenetic testing helped to improve the clinical outcome in virtually all children (95%, 19/20 children). Improvement (CGI-I) was 2 (0.79) (range 1-4): 2.1 (0.56) (range 1-3) in foster care children and 1.9 (0.99) (range 1-4) in non-foster care children. PGx testing helped reducing self-reported relevant side effects (p=0.006), the number of children on polypharmacy (from 65 to 45%) and the mean number of drugs per children (from 3.3 to 2.4 drugs, p=0.017).